
Watch this video to learn the proper mechanics to keep your back healthy while shoveling this winter!
Medical Articles & News
Watch this video to learn the proper mechanics to keep your back healthy while shoveling this winter!
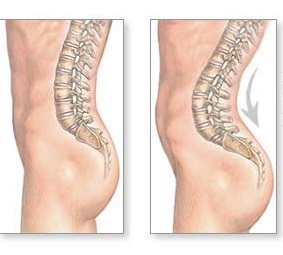
What is anterior pelvic tilt? APT is a change in posture that happens when the front of the pelvis drops forward, and the back of the pelvis rises. The condition pulls the abdominal muscles into a stretched position, which over time leads to a drastically weakened core. The glutes and hamstrings also suffer from being […]

Metabolic Resistance Training: Burn Fat and Build Muscle in Less Time! In about an hour, with lecture learn how to: Maximize Fat Burning and Muscle Building With a Short Session How MRT Enhances Muscles and Fat Loss, as well as Overall Health How to Set up Your Own MRT Training Sessions—Short Sweet and Highly Effective […]

A Client Testimonial. At AITC we are constantly working on providing the total approach to rehab, performance and overall fitness. As a result, the AITC and The Athletic Way teams collaborate and provide services for our patients and athletes including physical therapy, sports chiropractic, massage therapy and strength and performance training. Recently one of our […]
The elbow is a compound synovial joint. Three bones of the upper and lower arm make up the elbow joint – the humerus, radius, and ulna. The joint structure creates a triangular hollow called the cubital fossa on the front of the elbow. The elbow joint is protected by a capsule which surrounds it completely, […]

Snow has finally arrived and it’s time to break out the ice melt and shovels. Many of us may be familiar with the low back ache that can follow digging out from one of New England’s winter events. Engaging in snow shoveling is a complex activity that requires proper body mechanics and precaution. The constant, […]

The ankle is formed by the end of the shinbone and the outer leg bone over the talus. The subtalar joint in the ankle is formed by the underside of the talus and the top of the front part of the heel bone. The ankle is bound within a fibrous capsule which is lined by […]

We all know how important our feet are. They are keep us on the move and enable us to work, play, and function on a daily basis. The foot consists of many muscles, tendons, and twenty-six small bones. These bones are linked together as synovial joints, with capsules, ligaments, and synovial membranes. The ligaments which […]

Dynamic warm ups and static stretching are both part of injury prevention before and after activity. A dynamic warm up before activity uses stretches that are “dynamic,” meaning you are moving as you stretch. Dynamic stretching is ideal as the core of a warm-up routine for several reasons. It activates muscles you will use during […]

The hamstrings are three muscles which cover the back of your thigh, extending from your seat bone down to the back of your knee. They link the hip and knee joints. The sciatic nerve, which runs down the back of the thigh, supplies all three hamstrings. The hamstrings work concentrically to bend the knee and […]